Yellow fever
Yellow fever is an acute tropical disease, caused by an Arbovirus of the Flaviviridae family. First reported probably in the 17th century, the virus caused several serious epidemics that claimed many lives, including one in Livorno in 1804. Today it is found particularly in the tropical regions of Africa, and Central and South America.
It is such a serious, high consequence viral disease that several countries have made vaccination mandatory for all travellers arriving from at-risk areas.
CAUSES
The disease is caused by a positive single-stranded RNA virus that contains the virus genome; it belongs to the Flaviviridae family, of the genus Flavivirus. It is related to the Dengue, Zika and Japanese Encephalitis viruses.
Under an electron microscope, the virus appears as a spherical virion about 40 nm (nanometres) in diameter, with an icosahedral capsid (the outer wall of the virus), a characteristic of Flaviviruses. There is a lipid envelope, derived from the host cell, which contains two proteins E and M, which are critical for the virus’s access into host cells.
TRANSMISSION
The name of yellow fever comes from the yellow coloration of the eyes and skin as a result of the damage that the virus causes to the liver. The disease is transmitted through the bites of infected mosquitoes, of the genus Aedes (which transmit other diseases such as Zika, Chikungunya and Dengue) or Haemagogus, when they feed on human blood. Unlike the anopheles mosquito (a malaria vector), which is active at night, the Aedes mosquito also bites during the day.
Mosquitoes live and breed in tropical rainforests, humid and semi-humid environments, but also around bodies of stagnant water near human dwellings in urban environments. Increased contact between humans and infected mosquitoes, particularly in urban areas where people have not been vaccinated for yellow fever, can cause major epidemics.
The principal vector isAedes aegypti, which is found in Africa and South America, but mosquitoes of the genus Haemagogus are also present in the forests of South America. Aedes aegypti’s ability to establish itself in more temperate zones, like Europe, is currently limited due to its inability to survive harsher winters. This trend could reverse as a result of climate change.
Aedes albopictus is a species of mosquito found almost all over the world, including Italy, where it is commonly called the tiger mosquito. Although less effective than the other Aedes, the tiger mosquito can also transmit at least 22 arboviruses, including Yellow Fever, Rift Valley Fever, Dengue, Japanese Encephalitis, West Nile virus, Chikungunya, and Zika.
The virus enters the host cell via a mechanism called endocytosis, which is the process by which the cell engulfs the virus in its cytoplasm, where it is able to replicate. At that point it can infect other feeding mosquitoes that feed 2 days prior to the initial symptoms and up to 5 days after (it is not transmissible to people, however).
Epidemiologically speaking, the spread of the disease has two cycles:
- urban cycle: in this cycle the reservoir of the virus is humans; mosquitoes become infected by biting humans during the viraemic phase, i.e. the first 3 days of infection. Subsequently, the Aedes aegypti mosquito remains infected for life, transmitting the virus to both humans when it feeds and to its eggs.
- sylvatic cycle: in this case, mosquitoes contract the infection from infected monkeys or other primates, which act as reservoirs of the virus. Later, mosquitoes feed on humans which infects them.
Deforestation, climate change, increased incursions into forests and jungles for the purpose of mining, oil extraction, construction, and reclamation of farmland, are all phenomena that increase contact between humans and the mosquitoes responsible for the transmission of the yellow fever virus.
All these factors amplify the risk of contracting yellow fever, with urbanisation, large population movements, climate change, and increasing exposure of workers to infected mosquitoes in jungles and forests, all acting as primary drivers of the change in the epidemiology of the virus.
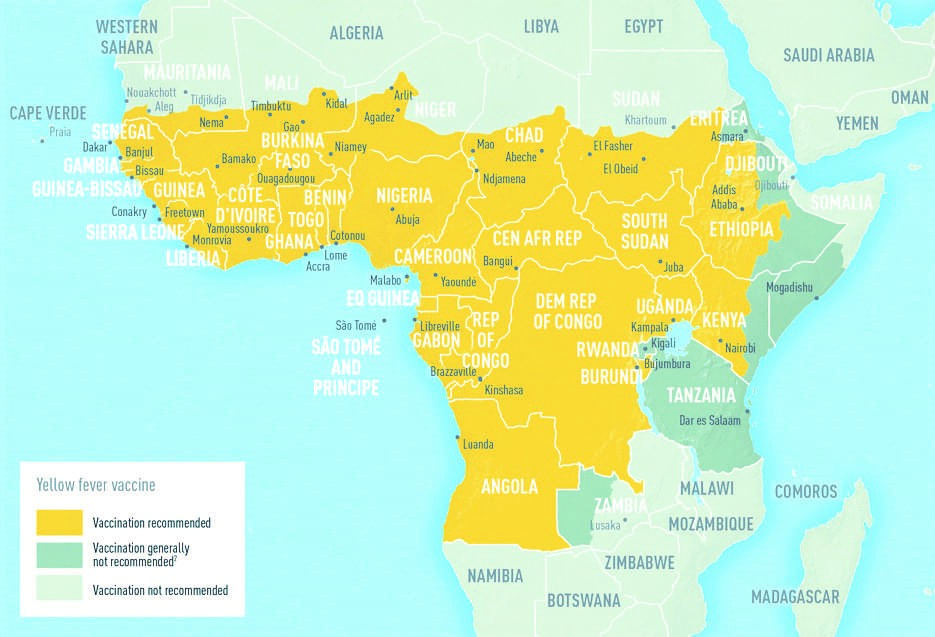
GEOGRAPHICAL DISTRIBUTION
Yellow fever is endemic in rural and humid areas, such as tropical forests. Most cases occur in sub-Saharan Africa and Central and South America, while in Asia the disease has never been reported.
Globally, 42 countries (29 in Africa and 13 in Central and South America)-are endemic or have endemic regions of yellow fever. Approximately 50 percent of infected individuals report no symptoms, which is precisely why the World Health Organization (WHO) estimates that 84,000 to 170,000 people are infected each year and about 29,000 to 60,000 die. However, as the infection originates in rural areas, the confirmed figures are always underestimated.
One of the major issues with yellow fever is the transfer of the disease beyond endemic regions. Occasionally, travellers to yellow fever endemic countries may carry the disease to countries that are free from yellow fever. In order to prevent said importation of the disease, many countries require a certificate of yellow fever vaccination before they will issue a visa, particularly when travellers are from or have visited areas where the disease is endemic.

SYMPTOMS
Symptoms of yellow fever generally appear 3-6 days after the mosquito bite. The infection can be completely asymptomatic, mild or very severe, and can even be fatal in some cases.
The symptoms of the disease can be divided into different stages:
- Onset of symptoms: in the early stage, symptoms are abrupt with extremely high fever (up to 39-40°C), headache, chills, rachialgia (pain in the spine), nausea and vomiting.
- The red stage: a few hours after the first symptoms, the red phase occurs. At this stage, the complexion of the patient’s face becomes bright red, with epistaxis, oliguria (low urine output) and persistent fever. This coincides with viremia (the presence of virus in the blood), which resolves within 3 days.
- Apparent remission: with a duration of approximately 24 hours.
- Yellow stage: the yellow stage appears around the fourth or fifth day of the disease, and is characterised by jaundice (yellowish discoloration of the skin), haemorrhage in various parts of the body and a persistent fever of approximately 40°C.
- Exitus: the stage when liver failure occurs, due to cytopathic damage and acute hepatic necrosis, as well as renal failure. Whereas, there is extensive bleeding in the intestines, melena (blood in stools), and vomiting, also known as “black vomit”.
- Healing: in some cases, after approximately 12-14 days of illness, patients can make a full recovery, without any significant damage to their organs, acquiring life-long immunity against the disease.
DIAGNOSIS
Particularly in the early stages, Yellow fever can often be confused with other diseases, such as malaria, dengue fever, and fulminant viral hepatitis. Consequently, diagnosis of the disease is not always obvious.
Diagnosis is confirmed by means of PCR (Reverse transcriptase-polymerase Chain Reaction), which can amplify the viral genome to identify the RNA of the virus. This technique is effective if it is used within the first few days of the onset of disease. Serological investigation is performed using the ELISA test to detect the presence of IgM antibodies, typical of a recent infection, which appear within the first 10-14 days of the disease. Finally, further laboratory analysis can identify abnormal levels of other relevant factors.
TREATMENT
To date, just like other infections caused by Flaviviruses, there is no specific treatment for yellow fever. Only supportive therapy is administered to relieve symptoms, such as dehydration, respiratory failure, and fever. In case of bacterial superinfection, antibiotics can be administered.
In endemic areas, the patient must be isolated to avoid further mosquito bites and, hence, block the chain of transmission.
PREVENTION
Preventive vaccination against yellow fever infection is the safest and most effective weapon against the transmission of the virus.
The vaccine is administered subcutaneously from the age of 9 months and over, as it is a live attenuated vaccine. WHO recommends a single dose of the vaccine, as one dose has been shown to provide life-long immunity.
Side effects are rare, although the risk is greater in individuals over 60 years of age, children under 9 months of age, pregnant women, and immunocompromised individuals. In each case, the risks and benefits should be evaluated, by assessing the risks of contracting the disease versus the possibility of post-vaccination adverse events.
The yellow fever vaccine has been used for many decades and is safe and affordable. It provides effective immunity against yellow fever in over 90% of vaccinated individuals within 10 days of vaccination, and 99% protection within 30 days of vaccination.
In addition to vaccination, people travelling to yellow fever endemic areas should adopt appropriate behavioural measures to prevent mosquito bites. These include: the use of mosquito repellents with approved efficacy and pyrethrum-based insecticides on clothing, suitcases, and in the corners of each room to prevent importation of any vectors on their return.
Bibliografy
Lin H. Chen e Mary E. Wilson, Yellow fever control: current epidemiology and vaccination strategies, Travel Medicine and Infectious Disease 10 (2020)
Moroni M., Spinello A., Vullo V. Manuale di Malattie Infettive. Edra LSWR, Masson, seconda edizione.
Bartolozzi G. Vaccini e Vaccinazioni, Seconda Edizione. Masson 2005.
Organizzazione Mondiale della Sanità (WHO): www.who.int
CDC Centers for Disease Center: www.cdc.gov


